
What is Robotic Partial Knee Replacement
It is the replacement of a part of the knee with the assistance of a robot.
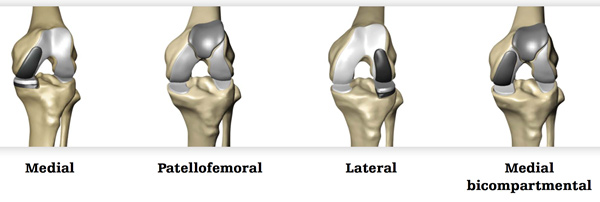
The Inner (medial), outer (lateral), front (patellofemoral) parts can all be replaced individually. Rarely a surgeon may want to replace 2 of the 3 parts at the same time (Bi-compartmental replacement).
How long has robotics been used to partial knee replacement
The first robotic partial knee replacement was performed in June 2006. Since then more than 50,000 procedures have been performed around the world. In Australia over 1000 procedures have been performed since its introduction in 2015. MHK surgeons first performed robotic Partial Knee replacements in 2016.
What is the revision (Redo) rate?
In 2017 the Australian Orthopaedic Associations National Joint Replacement Registry showed a 1-year revision rate of the MAKO partial knee replacement to be 0.8% which is the lowest of all listed prosthesis. The average for all partial knee prosthesis was 2.2%.
This is in keeping with previously published data for the Mako from the USA showing a 1.0% 2-year revision rate. When looking at traditional manual techniques in selected studies from specialist centers’ the 10-year revision rate for partial knee replacement may be as low as 2%.
There are is no long term data on survivorship of this procedure using a robot.
How is the operation planned?
The patients’ bony anatomy is registered during the operation which allows matching of the implant to the patients’ personal anatomy.
How is the operation performed?
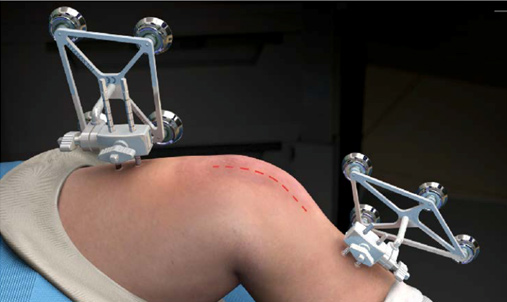
Small metal pins are attached to the leg and “trackers” or “arrays” will then tell the sensor where the leg is and when it is moved.
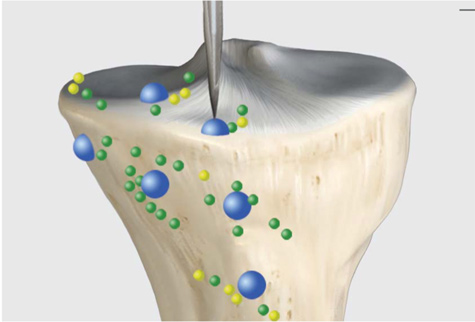
The patients’ anatomy is then checked and a series of points are registered to ensure the anatomy is matched to the CT scan.
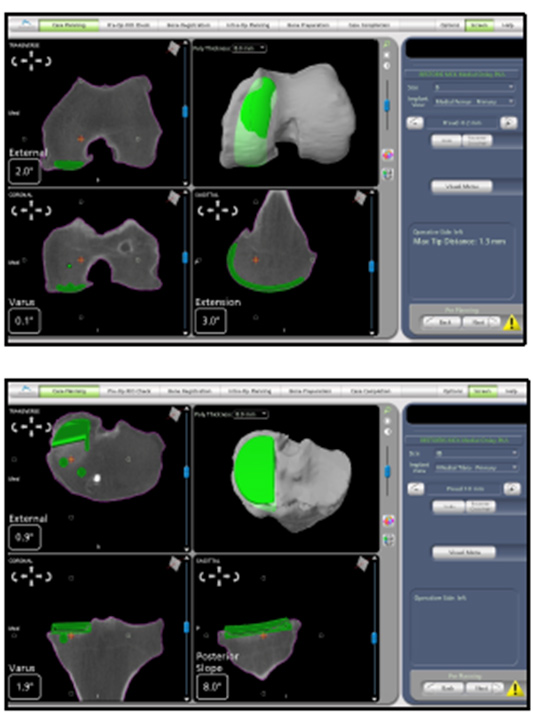
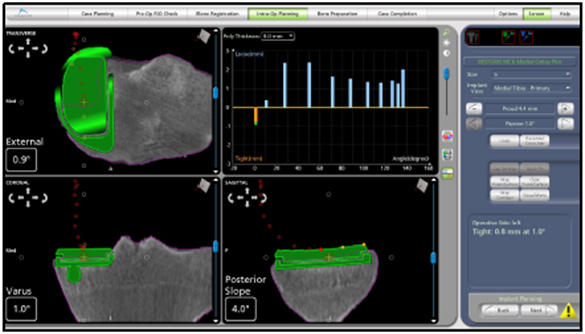
The knee is then put through a series of movements and the tension in the ligaments is measured and the movement of the knee is observed and the contact points between the components recorded. This produces a graph of the knee and a 3D model of how the knee will work after the replacement. The surgeon can then adjust the planned component position to change any aspect of the plan they want to improve.
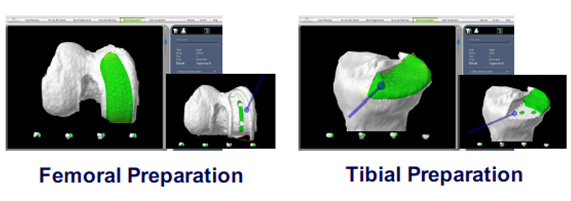
Once the plan is set the bone model is shown with an area highlighted in green which is the bone to be removed. The bur is then used by the surgeon to remove the bone but the robot doesn’t allow the bur to move outside of the plan making this a highly accurate procedure.
Is this a “less invasive operation”
NO.
While the main cut used may be slightly smaller than a standard operation there is no significant difference in wound size.
Is it more accurate
There have been studies which show improved accuracy using robotic for partial knee replacement. We hope that improved accuracy will lead to better outcomes for patients.
Our results with conventional partial knee replacements have been excellent, and because the non-robotic partial knee replacement has a 30-year track record, we are using robotic surgery for some, but not all, of our partial knee replacements.
- Achieving accurate ligament balancing using robotic-assisted uni-compartmental knee arthroplasty. Plate JF1, Mofidi A, Mannava S, Smith BP, Lang JE, Poehling GG, Conditt MA, Jinnah RH. Adv Orthop. 2013;2013:837167. doi: 10.1155/2013/837167. Epub 2013 Mar 24.
- Accuracy of Dynamic Tactile-Guided Uni-compartmental Knee Arthroplasty, Dunbar, Nicholas J. et al. The Journal of Arthroplasty, Volume 27, Issue 5, 803 - 808.e1
- Improved Accuracy of Component Positioning with Robotic-Assisted Uni-compartmental Knee Arthroplasty, Stuart W. Bell, Iain Anthony, Bryn Jones, Angus MacLean, Philip Rowe, Mark Blyth. J Bone Joint Surg Am Apr 2016, 98 (8) 627-635; DOI: 10.2106/JBJS.15.00664
- Yildirim G, Fernandez-Madrid I, Schwarzkopf R, Walker PS, Karia R. Comparison of robot surgery modular and total knee arthroplasty kinematics. J Knee Surg. 2014 Apr;27(2):157-63.
- In vivo kinematics of a robot-assisted uni- and multi-compartmental knee arthroplasty. Watanabe T1, Abbasi AZ, Conditt MA, Christopher J, Kreuzer S, Otto JK, Banks SA. J Orthop Sci. 2014 Jul;19(4):552-7. doi: 10.1007/s00776-014-0578-3. Epub 2014 May 2.
- Koskinen E1, Eskelinen A, Paavolainen P, Pulkkinen P, Remes V. Comparison of survival and cost-effectiveness between unicondylar arthroplasty and total knee arthroplasty in patients with primary osteoarthritis: a follow-up study of 50,493 knee replacements from the Finnish Arthroplasty Register. Acta Orthop. 2008 Aug;79(4):499-507.
- Short to Mid Term Survivorship of Robotic-Arm Assisted Unicompartmental Knee Arthroplasty Thomas Coon, MD, Martin Roche, MD, Andrew Pearle, MD, Jon Dounchis, MD, Todd Borus, MD, Frederick Buechel, MD, Manoshi Bhowmik-Stoker, PhD, Michael Conditt, PhD 17th EFORT Congress 2016 Geneva, CH, 01-03 June
- Accuracy of UKA Implant Positioning and Early Clinical Outcomes in a RCT Comparing Robotic Assisted and Manual Surgery. Iain Anthony, Bryn Jones, Angus MacLean, Philip Rowe, Mark Blyth. University of Stracthclyde and Glasgow Royal Infirmary.
- Arno, S; Maffei; Walker, PS; Schwartzkopf, R; Desai, P; Steiner, GC. Retrospective Analysis of Total Knee Arthroplasty Cases for Visual, Histological and Clinical Eligibility of Unicompartmental Knee Arthroplasties. J. Arthorplasty. 2011. 26(8): 1396-1403